Non-Surgical Treatment for Spinal Stenosis Is Successful
Primarily, spinal stenosis affects patients over 50 years of age, and it really affects more and more people at 60, 70, and 80. It's been reported that 1 in 200 people over age 50 have spinal stenosis. (1) One report states that 100% of 33 asymptomatic persons -- persons reporting no pain -- over 55 years old have lumbar spinal stenosis. (2) Could you be one of the patients with spinal stenosis in Augusta?
Spinal Stenosis Care Options in Augusta: Surgical vs. Non-Surgical
Medical and chiropractic research supports the use of conservative, non-operative, non-surgical treatment for spinal stenosis when possible. Chiropractic is conservative care. chiropractic is non-surgical. Why conservative, chiropractic care for spinal stenosis? Read on.
chiropractic Spinal Stenosis Care
Medical researchers call for "aggressive, non-surgical care" for stenosis. (14) Offered at Lombardy Chiropractic Clinic, the Cox Technic system of protocols for spine pain relief has published guidelines for care and relief expectations. Lombardy Chiropractic Clinic adheres to these guidelines to aggressively manage back pain non-surgically. Both of us - the doctor and the patient - play important roles in healing: appointments, treatment, exercise, nutrition, ergonomics, etc.
As a viable, non-surgical treatment option for spinal stenosis, Lombardy Chiropractic Clinic's Cox Technic chiropractic flexion-distraction and decompression is gentle, doctor-monitored, safe spinal manipulation offering these benefits:
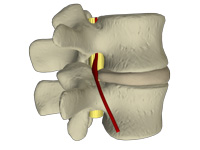
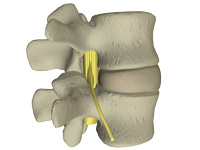
- opening of the stenotic spinal canal space by 28% (13)
- dropping intradiscal pressure (13)
- re-aligning the facet joints and re-storing motion to the joints to the best of their ability
There is hope for relief and control of your pain even when stenosis and disc degeneration narrow the spinal space. Lombardy Chiropractic Clinic offers Cox Technic flexion distraction and decompression to help you avoid the extra emotional - frustration over not getting the help you need or enough relief to regain your quality of life - and financial costs associated with dealing with spinal stenosis in Augusta.
Cost of Spinal Stenosis
Spinal stenosis treatment is expensive whether you have spinal stenosis in Augusta or elsewhere. Options for managing spinal stenosis are non-surgical and surgical; however, comparing the outcomes and costs is enlightening.
In a 3-year study of Medicare patients treated surgically and non-surgically (9), it is reported that the
- surgery patients cost $49,624
- non-surgery patients cost $36,691
In another study (4), the adjusted mean hospital charges for two types of surgical procedures were
- $80,888 for complex fusion procedures
- $23,724 for decompression alone.
Researchers found that from 2002-2007 (4)
- the rate of complex fusion procedures increased 15 times - from 1.3 to 19.9 per 100,000 beneficiaries.
- life-threatening complications increased with increasing surgical invasiveness, from 2.3% among patients having decompression alone to 5.6% among those having complex fusions.
Surgery for leg pain (radiculopathy) with herniated lumbar disc and symptomatic spinal stenosis is associated with short-term benefits compared to non-surgical therapy, but benefits of the surgical care diminish with long-term follow-up (5)
Non-surgical options cost less.
Surgery or No Surgery for Augusta Spinal Stenosis? Try No Surgery First
Which is right for you? Consider these reports:
Lumbar spinal stenosis patients over 70 with radicular symptoms are good candidates for conservative treatment as long as complete myelographic block is not present. (6)
Atlas et al's 8 to 10 year follow up study (7) revealed nearly the same outcomes in surgically and non-surgically treated stenosis patients who reported that their predominant symptom of low back pain was improved: 53% of surgically treated and 50% of non-surgically.
- Both groups were satisfied with their current status:
- 55% of surgically treated stenosis patients
- 49% of non-surgically treated stenosis patients.
Spinal manipulation is recommended by The American Pain Society and the American College of Physicians for primary care of low back pain. (10)
Washington state Worker's Compensation data from 1994 to 2001 compared lumbar fusion with cages and instrumentation to non-surgical care in 1950 subjects (11):
- Lumbar cage fusion rates increased from 3.6% in 1996 to 58% in 2001
- Result was increased complication risk without improving disability or reoperation rates.
- 2 years after fusion
- 64% disabled
- 22% re-operation
- other complications 12%
- 2 years after fusion
- Lumbar fusion devices compared with exercise and cognitive intervention are no better.
- Use of cages or instrumentation was associated with increased complication risk compared with bone-only fusions without improving disability or re-operation rates.
- Use of intervertebral fusion devices rose rapidly after their introduction in 1996.
- This increased use was associated with an increased complication risk without improving disability or reoperation rates.
A study of Worker Compensation patients with chronic low back pain was conducted from January 1999 to December 2001. The randomly selected patients were followed through January 2006. The results were not favorable for surgery. (12)
- 725 lumbar fusion cases were compared to 725 controls who did not undergo surgery.
- BETTER NON-SURGICAL RETURN TO WORK STATISTICS
- 2 years after fusion surgery:
- Only 26% of fusion cases had returned to work
- 67% of non-surgical controls had returned to work
- 2 years after fusion surgery:
- Re-operation Rate: 27%
- Surgical Complications: 36% of lumbar fusion subjects
- LOWER Non-Surgical Permanent Disability Rates
- 11% for surgical cases
- 2% for non-operative controls.
- LESS Non-Surgical Drug Use
- among lumbar fusion surgical patients:
- 41% increased daily opioid drug use after surgery
- 76% of cases continuing opioid drug use after surgery.
- among lumbar fusion surgical patients:
- FEWER Non-Surgical Patient Days Off Work
- Total number of days off work was more prolonged for surgical cases:
- 1140 days for surgical
- 316 days for non-surgical
- Total number of days off work was more prolonged for surgical cases:
The Augusta chiropractic Option
Cox Technic drops intradiscal pressure, widens the spinal canal area and increases intervertebral disc height to reduce stenosis and relieve stenosis pain.
Contact Lombardy Chiropractic Clinic in Augusta for chiropractic Cox Technic Flexion Distraction and Decompression for relief of your spinal stenosis. Lombardy Chiropractic Clinic offers a thorough examination, consultation and treatment plan to relieve and control your spinal stenosis pain without surgery if possible.
- FreeMD - http://www.freemd.com/spinal-stenosis/incidence.htm
- Tong, HC; Carson, JT; Haig, AJ; Quint, DJ; Phalke, VR; Yamakawa, KSJ; Miner, JA: Magnetic resonance imaging of the lumbar spine in asymptomatic older adults. Journal Of Back And Musculoskeletal Rehabilitation 2006;19 (2-3). 2006. p.67-72
- Simon JE: Discogenic disease of the cervical spine. Sem in Roentgenology Vol XXIII
- Deyo RA, Mirza SK: Trends, Major Medical Complications, and Charges Associated With Surgery for Lumbar Spinal Stenosis in Older Adults. JAMA. 2010;303(13):1259-1265
- Chou R et al: Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain An Evidence-Based Clinical Practice Guideline From the American Pain Society. SPINE 2009;34 (10):1066-77
- Tadokoro, K: et al: The prognosis of conservative treatments for lumbar spinal stenosis: analysis of patients over 70 years of age. Spine 2005; 30(12):2458-63
- Atlas SJ, Keller RB, Su YA, Deyo RA, Singer DE: Long Term Outcomes Of Surgical And Nonsurgical Management Of Lumbar Spinal Stenosis: 8 To 10 Year Results From The Maine Lumbar Spine Study. Spine 2005;30(8):936-43
- Murphy DR, Hurwitz EL, Gregory AA, Clary R: A non-surgical approach to the management of lumbar spinal stenosis: A prospective observational cohort study. BMC Musculoskeletal Disorders 2006 7: NIL_1-NIL_8
- Chen E, Tong KB, Laouri M: Surgical treatment patterns among Medicare beneficiaries newly diagnosed with lumbar spinal stenosis. Spine J. 2010 Jul 10, (7):588-94. Epub 2010 Apr 8.
- Chou R et al; Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain An Evidence-Based Clinical Practice Guideline From the American Pain Society. SPINE 2009;34 (10)1066-77
- Juratli S, Franklin G, Mirza S, Wickizer T, Fulton-Kehoe D: Lumbar Fusion Outcomes in Washington State Workers' Compensation. Spine 2006; 31(23):2715-2723
- Nguyen TH, Randolph DC, Talmage J, Succop P, Travis R: Long-term Outcomes of Lumbar Fusion Among Workers' Compensation Subjects: An Historical Cohort Study. Spine 2010, post author corrections, 23 August 2010
- Cox JM: Low Back Pain. 6th ed. Philadelphia: Lippincott Williams and Wilkins, 1999. Appendix B by Ram Gudavalli PhD.
- Simotas AC, Dorey F, Hansraj K, Cammisa F: Non operative treatment for lumbar spinal stenosis: clinical and outcome results and a 3 year survivorship analysis. Spine 2000;25(2):197-203